Del:
Take it offline!
This Education in Motion resource is also available as a printable PDF.
Last ned PDF
When the rear axle is set correctly for a self-propelling manual wheelchair user the wheelchair feels better and opens up the most independent performance. Set poorly and the wheelchair can become unstable, painful and even more immovable than the current parliamentary Brexit debate.
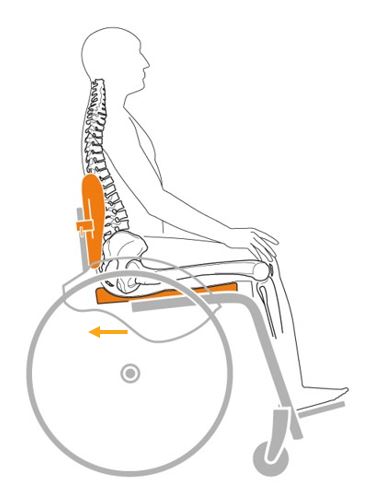
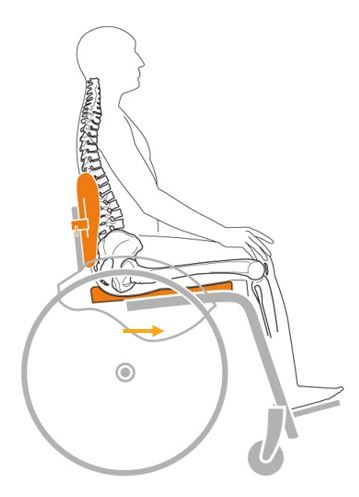
One of the first concepts most high-end manual wheelchair prescribers learn is that, generally, moving the rear axle forward makes propulsion easier but reduces the rear stability. This isn’t inherently a bad thing, as a little rearward ‘tippiness’ is needed to clear small everyday obstacles.
An oft-quoted guideline for users with moderate or high level self-propulsion skills is to set the rear axle centre at the tip of the client’s middle finger. This meets the needs of most wheelchair users with moderate manual mobility skills and typical centre of mass, that is, it works fairly well for people who are somewhere near the proportions of an average crash test dummy. But, what to do when this might not be a good starting point?
1. User’s own centre of mass is quite rearward
- Amputees, particularly double amputees
- Petite clients with very little weight held in their abdomen, chest, thighs and lower limbs
- Clients who hold most of their soft tissue mass in their gluteal area, particularly if combined with one or more of the above
Solution: Start with a more conservative setting, but with caution. The farther back a rear axle setting goes, the more hyperextension of shoulder is needed to propel, which can make propelling inefficient and increase the risk of upper limb trauma such as repetitive strain injury. Try in line with backposts is a good place to start and ensure you order a very configurable wheelchair. Even with a relatively rear set personal centre of mass, some clients can tolerate a more active position. For amputees who have the ability to develop wheelchair mobility skills we would recommend starting here and considering 2x anti-tips and additional training.
2. User’s own centre of mass is quite forward
- Clients with large amounts of weight held in lower limbs, such as clients with chronic oedema
- Clients with very little rear gluteal mass, particularly in combination with large chest, abdominal or lower limb soft tissue mass.
Larger clients are particularly likely to have forward centres of gravity, and therefore load the front castor wheels heavily if they do not have a forward set COG. Unfortunately heavy duty chairs sometimes have even less ability to bring the COG setting forward! Suggest going brave, with axle position an ‘active’ position of approx. 5 cm in front of the backposts, even on moderate or low active users, again with anti-tippers if needed initially until confidence is built up. This is even more important if a carer assists and has to tip the front castor wheels up over thresholds, to push the chair.